Cerebral Palsy
Early diagnosis can help leading active and self supporting lives
Dr Selina Daisy
Cerebral palsy (CP) is a condition that affects thousands of babies and children each year. It is not contagious. Cerebral palsy means the disorder of the brain, mainly due to brain damage occurring before birth, or due to lack of oxygen during birth resulting in weakness or problem in the way a person moves or positions his or her body. Normally the brain tells the rest of the body exactly what to do and when to do it. Since CP affects the brain, depending on what part of the brain is affected, a kid may not be able to walk, talk, eat, or play the way most kids do. It is a non-progressive but often changing motor (referring to movement or which produces movement) impairment syndrome. The changing clinical picture results from developmental maturation and intervention. Signs and symptoms
Symptoms of cerebral palsy can be as simple as having difficulty with fine motor tasks like writing or using scissors, or as profound as being unable to maintain balance or walk. Severely affected patients may have involuntary movements, such as uncontrolled motion of hands and drool. Others suffer from associated medical disorders, such as seizure (convulsion), speech problem, hearing problem, language disorder, ocular problem (i.e. squint, refractory errors, fields defects etc.), feeding difficulties, behavioral problems and mental retardation. Types
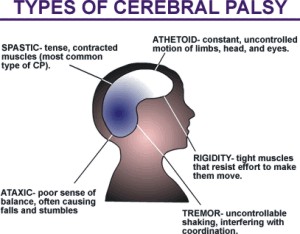
It can be classified mainly into two categories: physiologic and topographic. Spastic CP is the most common type of cerebral palsy. It causes the muscles to be stiff and permanently contracted. Spastic cerebral palsy is often sub classified as one of five types that describe the affected limbs. Spastic diplegia (paralysis of a similar part on both sides of the body) affects legs more than arms. The legs often turn in and cross at the knees. This causes a scissors gait, in which the hips are flexed or bent, the knees nearly touch, the feet are flexed, and the ankles turn out from the leg, causing toe-walking. Learning disabilities and seizures are less common than in spastic hemiplegia. Spastic quadriplegia involves all four limbs. There is dysfunction of the muscles of the mouth and tongue, seizures, medical complications and increased risk for cognitive difficulties. Dyskinetic cerebral palsy is characterised by slow, uncontrolled, writhing movements of the hands, feet, arms, or legs. Patients also may have abrupt, irregular, jerky movements or slow rhythmic movements with muscle tone abnormalities and abnormal postures (dystonia). The muscles of the face and tongue may be affected, causing grimacing and/or drooling. When the muscles that control speech are affected, the patient experiences dysarthria (abnormal pronunciation of speech). Hearing loss is commonly associated with this form of CP. Hypotonic cerebral palsy characterised by marked motor delay and decreased tone. Often confused as a floppy infant. Ataxic cerebral palsy affects balance and depth perception. Persons with ataxic CP have poor coordination and walk unsteadily, usually placing their feet far apart. Many have trouble with quick or precise movements, like writing or buttoning a shirt. Some also have intention tremor, in which a voluntary movement, like reaching for an object, sets off trembling in the limb. Mixed CP involves two or more types of cerebral palsy. While any mix of types and subtypes can occur. A kid with CP may present mild to server symptoms depending on how much of the brain is affected and which parts of the body that section of the brain controls. No one knows for sure what affects the most. For some babies, injuries to the brain during pregnancy or soon after birth may cause CP. Sometimes the problem in the brain occurs before the baby is born. Complications
Some people with CP have associated disorders like impaired intellectual development, seizures, failure to grow and thrive, vision and sense of touch problems. As many as half of all patients with cerebral palsy have seizures. Seizures that recur without a direct trigger, such as a fever, are classified as epilepsy. Children with moderate-to-severe cerebral palsy, especially those with spastic quadriplegia, often experience failure to grow or thrive. Infants fail to gain weight normally; young children may be abnormally short; and teenagers may be short for their age and may have slow sexual development. These phenomena may be caused by a combination of poor nutrition and damage to the brain centers that control growth. Some patients, particularly those with spastic hemiplegia, have muscles and limbs that are smaller than normal. Limbs on the side of the body affected by CP may grow slower than those on the other side. Hands and feet are most severely affected. Vision and hearing problems are more common in people with cerebral palsy than in the general population. Differences in the left and right eye muscles often cause the eyes to be misaligned. Strabismus can lead to poor vision and impaired depth perception, some physicians recommend corrective surgery. Diagnosis
The diagnosis of CP is essentially clinical. It involves detail history of prenatal, natal and postal history and careful physical and neuro-developmental examination to identify deficit type and topography (description of each particular part of the body), which is required for management. Importance of early diagnosis
Early identification has significant implication for the family and necessitates early intervention to achieve the maximum holistic potential of the child. The philosophy behind early intervention is based on the following facts: A neurological insult recovers better with stimulation. IQ of emotionally deprived children is poorer than stimulated children. The plasticity of the brain in the first decade of life provides a window of opportunity for active intervention. Actually a child with CP is not hopeless. Half of the child with CP have average or above IQ. With timely medical care and proper guidance, a vast majority can lead active, self supporting lives. Thus early diagnosis is prerequisite. The writer is an Associate Professor of Pediatric Neurology and Clinical Neuro-physiology of Dhaka Medical College, Dhaka.
|