State of Tuberculosis in Bangladesh
BRAC Bangladesh and The Daily Star jointly organized a roundtable discussion on the “State of Tuberculosis in Bangladesh” on 13 December 2005, at the Seminar Room of The Daily Star. The objective was to explore the situation of TB in the country and the various efforts to battle it by different partners and stakeholders. It was expected that useful recommendations would also emerge from the meet. Participants were from various TB partnership agencies including the Government of Bangladesh, NGOs, health providing and research agencies, donors and other international agencies as well as public health specialists and health practitioners. Most of the participants at the meet had been active in the past few years in the National TB control programme, which is the key thrust programme to combat the virulence of TB in Bangladesh.
The meeting was introduced by the host Mr. Mahfuz Anam, Editor and Publisher of “The Daily Star”. He said that The Daily Star has always cooperated with wider civil society initiatives on critical issues like combating TB and this was such a case. Mr. Abdul- Muyeed Chowdhury, Executive Director of BRAC, who presided over the meeting, said that a scourge like TB could not be controlled unless there was serious collaboration and sharing of experiences like this meeting. After this the guidelines for conducting the workshop was spelt out by the Editor. Next, the participants introduced themselves and the meeting began. The roundtable had two parts: Presentation and Open discussion
Abdul Muyeed Chowdhury, Executive Director, BRAC: Bangladesh is an over-populated country and very vulnerable to tuberculosis. It is a major public health problem of the country. Based on current estimates, approximately 300,000 people fall ill due to Tuberculosis and 70,000 die of the disease every year. In order to control Tuberculosis effectively, Bangladesh is implementing the WHO recommended Directly Observed Treatment Short Course (DOTS) strategy. Bangladesh is trying to establish a Public-Private Partnership for controlling Tuberculosis through an outreach network of diagnostic and treatment facilities. BRAC is also one of the partners with other NGOs and civil society members and is working closely with the National Tuberculosis Control Programme of the Government as part of the partnership.
At present, the tuberculosis control programme is working much better than before and improvements can be easily sighted. In the year 2000, the case detection rate of TB was 30%. This went up to 46% in 2004. It expected to go up to 65% by the next year (2006). In the areas covered by BRAC this has already reached 65%. The national average cure rate is 86%; in BRAC covered areas it is 89%. The Public Private Partnership can thus bring about a major change in the situation both at the national and the local level.
Community involvement is a key factor here and BRAC is implementing the programme using community involvement through the Shasthaya Shebika. They are field level para-volunteers who ensure daily intake of medicines and are paid a small sum of money to do this critical task. They represent the community spirit and willingness of the people to participate at the village household level to ensure health for all.
MULTIMEDIA PRESENTATION
After the initial remarks by the Chair, Dr. Vikarunnessa Begum, Programme Manager, National Tuberculosis NTP, DGHS gave a brief multimedia presentation on the “Tuberculosis Control Programme of Bangladesh”.
I am going to present an outline of the National Tuberculosis Programme in Bangladesh. But before going to that, I would like to say a few words about the TB situation in some other countries.
About one-third of the world's population is infected with tuberculosis. More than ten people are infected by TB every day and three million die of it each year. TB is more prevalent in males that in females and it is the widest cause of maternal death.
In most cases, TB occurs in the 15 45 age groups. Twenty-two countries constitute 85% of the TB burden in the world. Three countries (India, China and Bangladesh) are among the five high burden countries in south-east Asia and Bangladesh is one of the top 5 high burden countries in the world.
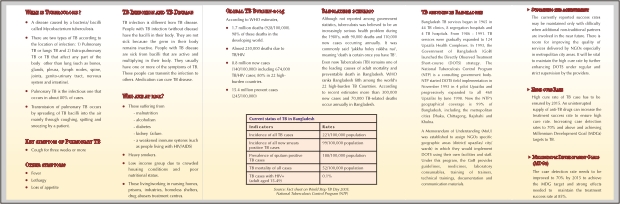
TB estimates in Bangladesh of 2004 say that about 50% of the adult population are infected by TB and there are 221/10000 population: incidence of new TB cases (all form) per year with one new TB case every 2 minutes and one TB death every ten minutes. Each year about 70,000 people die from TB in Bangladesh.
The vision and mission of the NTP are to battle Tuberculosis, as it is a major public health problem in Bangladesh. NTP's mission is to strengthen the effort of TB control through effective partnership, mobilizing resources and ensuring quality diagnostic and treatment services under the Directly Observed Treatment Short Course (DOTS) strategy. Also, the service should be equally available to all people of Bangladesh irrespective of age, sex, religion, ethnicity, social status and race.
The objectives for the mission is to sustain the 2005 targets achieving at least 70% case detection and 85% treatment success among TB cases under DOTS. To meet the objective and to control the crisis of TB problem, NTP proposes DOTS strategy which has five components:
I. Government commitment: to ensure necessary political and financial support.
II. Case detection through sputum microscopy: cost effective diagnosis focus on smear positives, passive case finding, direct microscopy of sputum for AFB.
III. Short-course Chemotherapy: effective treatment of the TB short course, standardized, multi drug, Directly Observed Treatment (DOT). Cure is the best prevention.
IV. Supply system: to ensure uninterrupted supply of drugs and lab reagents.
V. Recording and reporting: to follow the patient and monitor the progress of treatment; standard forms, cards and registers; cohort analysis.
To ensure DOT, every Upazilla Health Complex is facilitated with DOTS. We have NGO facilities and better collaboration with GoB and NGOs at the local level. We can ensure it by involving NGO workers and community members. In severe cases the patient has the provision to get admitted to the hospital. If community based DOTS is not possible, it can be ensured by offering family DOTS.
There have been 14 important achievements -- See Box for 14 achievements -through out Bangladesh by taking different initiatives in this programme. The date shows the situation regarding case detection and treatment success rate between the years 1993 2004. The case detection rate for 2004 was 46% and treatment success was 80.6% - 85%. It is expected that at the end of 2005, case detection will rise to around 60%.
Some of the challenges of NTP faces today are:
- Implementing health sector reform and integrating TB programmes within that. (Health, Nutrition and Population Sector Programme);
- Effective partnership with private sector, academic institutes and workplaces in DOTS expansion;
- Capacity development for effective supervision, monitoring and quality control;
- Adequate central level staff to carry out the programme smoothly;
- Appropriate initiatives for ACS (Advocacy, Communication and Social Mobilization).
By meeting these challenges hopefully we can reach the 70% target case detection by the next year (2006).
NTP achievements at a glance
1. Expansion of DOTS in Dhaka and other City Corporations
2. Introduction of DOTS in prisons, academic institutions and workplace
3. Sustaining strong collaboration between Government & Non-Government organizations
4. Access to the Global DOTS Expansion plan funded by CIDA, Global Drug Facility (GDF), Global Fund to Fight AIDS, TB & Malaria (GFATM) and strong technical support from WHO
5. Initiation of Public Private Partnership Pilot Project in Dhaka City and process of linkage with NTP-NGOs
6. Detection of estimated new smear positive cases under NTP increased to 46% in 2004 as compared to 34% in 2002, expected detection rate over 55% in 2005.
7. Expansion of External Quality Assurance of smear microscopy
8. Revision, printing and distribution of laboratory guidelines
9. Revision of National guidelines, incorporating the new regimens including FDCs
10. Establishment of TB Steering Committee, Training Working Group
11. Confirmation of funds for TB prevalence study
12. NTP implementing different operational research jointly with ICDDR,B and other International organizations with publications in journals
13. Awareness campaigns initiated through mass media
14. Steps taken to function DRS
Participants
Professor Dr. M. Amanullah, MP, Member, Parliamentary Health Standing Committee
Dr. Tahmina Aziz, Director ( MBDC & Line Director-TB & Leprosy control program )
Dr. Vikarunnessa Begum, Program Manager, TB, NTP
Maj. Gen (Dr.) ASM Matiur Rahman, Chief Advisor, National HIV/AIDS program
Professor Md. Mostafizur Rahman, Director, NIDCH
Mahfuz Anam, Editor, The Daily Star
Abdul-Muyeed Chowdhury, Executive Director, BRAC
Dr. Salehuddin Ahmed, Pro-Vice Chancellor, BRAC University
Dr. Zafrullah Chowdhury, Projects' Coordinator, Gonoshasthaya Kendra(GK)
Dr. Marijke Becx-Bleumink, MO-TB, WHO, Dhaka, NTP
Rachel Gugielmo, Project Director, Open Society Institute
Emilly Bell, Project Officer, Open Society Institute
Dr Frank Paulin, Health Advisor, DFID
Dr. Peter Herzig, Health Advisor, Delegation of the European Commission
Dr. Dinesh Nair, Health Specialist, World Bank
Dr. Shaila Rodrigues, Second Secretary (Development), Canadian High Commission
Dr. Khandoker Ezazul Haque, National Consultant, WHO, NTP
Robert J. Timmons, Chief of party, NSDP
Dr. Mirza Mohammad Hiron, Associate Professor, NIDCH
Dr. Asif Mujtaba Mahmud, Associate Professor, Respiratory Medicine, NIDCH
Dr. A. K. Md. Ahsan Ali, Chief Organizer, Public Private Partnership Pilot Project
Dr. Md. Abdul Hamid Salim, Country Director, Damien Foundation
Dr. Ubaidur Rob, Country Director, Population Council
Dr. Sakhawat Hossain, Secretary General, NATAB
Dr. Nasir Uddin, Adviser, NATAB
Shaikh Abdud Daiyan, Mnaging Director, Grameen Kalyan
Mohammad Iqbal, Project Director, UPHCP
Professor AKM Shamsul Haq, Former Director, NIDCH
Dr. Sadia Dilshad Parveen, Director, Quality Improvement, NSDP
Faruque Ahmed, Director, BRAC Health program (BHP)
Afsan Chowdhury, Director, BRAC Advocacy and Human Rights Unit
Dr. K. Zaman, Scientist/ Epidemiologist, ICDDRB
Dr. Makhduma Nargis, Vice-President, Bangladesh Mohila Parishad
Dr. Hassan, TB Coordinator, NSDP
Dr. Md. Akramul Islam, Program Manager, BRAC Health program
Runia Mowla, Coordinator, En Gender Health, Bangladesh Country Office
Md. Rajib, Reporter (Health Page), The Daily Star
Moazzem Hossain, Staff Corespondent, Daily New Age
Maruf Ibne Mahbub, Reporter, Daily Prothom Alo
Dr. Mahfuza Rifat, Training Specialist, BRAC Health program
Irene Z. Zaman, Communication Specialist, BRAC Health program
Dr. Israt Nayr, Medical Officer, BRAC Health program
SK. Mojibul Huq, Field Communicator, BRAC Advocacy and Human Rights Unit
Mohammed Hasan Mahmud, MIS Analyst,BRAC Health program
Mahfuza Jasmine, Field Communicator, BRAC Advocacy and Human Rights Unit
Farzana Sultana, Field Communicator, BRAC Advocacy and Human Rights Unit
Syeda Jamila Siddika, Field Communicator, BRAC Advocacy and Human Rights Unit

DISCUSSION
Prof. Dr. Mirza Mohammad Hiron, Associate Professor, National Institute of Diseases of Chest and Hospital (NIDCH); BRAC has implemented the DOTS Programme through the Shasthaya Shebika, but it is really the job of doctors. For proper treatment and diagnosis, trained doctors and technicians are essential.
More then 30 million new infected cases occur in this country every year, and 70,000 people are killed by Tuberculosis every year. This is the fixed scenario from 1993. Though NTP (National Tuberculosis Programme) started TB control programme to stop new cases of infections, the figures remain the same since 1993.
Regarding the dual figures of case detection rate between the NTP and BRAC, I see that the case detection rate of NTP in 1993 and 1994 was 0.1 and 1.2 respectively but according to BRAC this figure is 26 and 29 in 1903 and 1994 respectively. This needs some clarification.
Dr. Vikarunnessa Begum, Programme manager (TB), TB and Leprosy Control Program; Let me answer the question of data and figures. BRAC estimates are only for the particular region where they operate but NTP focuses on the whole of Bangladesh. In case of 0.1% case detection rate in 1993, we had only just started the NTP programme and were very new in that field. Which is why the achievement rate was described as so low. It's a baseline figure.
Major General Dr. A.S.M Motiur Rahman (Rtd.), Chief Advisor of national HIV/AIDS programm and Chairman, Technical committee, National Aids Committee: Bangladesh is suffering from three major problems. They are malnutrition, infection and over-population. Such problems are largely associated with illiteracy, ignorance, poverty and superstition. In order to control Tuberculosis, which is a national problem and makes us most vulnerable, we have to first fight social problems.
Our immediate priority should be increasing the rate of Tuberculosis case detection. Tuberculosis case detection rate must be increased to 60% by utilizing advanced technology, sputum microscopy and ensuring availability of drugs.
I will emphasize on the efficient utilization of money from donor groups, such as the US$44 million for TB control programme. Proper utilization of money would be very important for us.
Dr. Marijke Becx-Bleumink, MO-TB, WHO: The total number of patients has been decreasing in the last few years due to different activities initiated for preventing TB in the country. It is not easy to estimate the actual number of cases. Prevalence survey can be much more accurate to estimate the case detection and treatment services. That may account for any statistical discrepancy. However, the programme has been able to make progress despite many obstacles. Conducting a prevalence survey is being considered.
Dr. Ahsan Ali, Chief organizer, Public Private Partnership Pilot project: NTP programme's objective is to cut down the chain of infection and to ensure treatment for TB patients. NTP's next target is to explore the unexplored cases, the left outs, who should be registered. There may also be problems concerning patients not under the umbrella of the national programme. About 60% to 70% patients go to private practitioners at the initial stages. Those private practitioners handle the cases as they best deem fit and they are not registered in the NTP's data base. For removing this problem, I propose strengthening of the Public Private Partnership.
I would also like to focus on community awareness. It is very important to ensure that people to go to public healthcare centres. Community awareness can be ensured through more advocacy activities. It should be aimed not only at the client or community level but also civil society at large.
Dr. M. A. Hamid Salim, Country Director and Medical Advisor, Damien Foundation: The major problem in Bangladesh is the failure of root case finding. At the public level, we have the facilities of free treatment, free drug, free diagnosis and free case finding facilities, but we could not achieve our desired result. There are some other issues related with the TB controlling programme. I'll mention two specific issues related with the TB control programme:
1. Social Awareness: Since the extreme poor of the society have no access either to the media or the health education programme, they are living beyond the information net Thus they have no idea about TB treatment which is free of cost.
2. Private Sector: Although many people go to private practitioners, about 30% do not comply with the treatment. We must ensure DOTS in every case. Every public and NGO programme must have a strategy to introduce DOTS to the general people and also ensure free treatment and diagnosis facilities in every Upazilla and Union. Both public and private partner should come closer to eliminate this problem but it is the public sector that has to provide free treatment facilities to the people, not the private sector.
Dr. A.K.M. Shamsul Haq, Former Director, National Institute of Diseases of Chest and Hospital: We are trying to make DOTS programme successful but unfortunately we cannot maintain 100% DOTS in every cases. It is also not possible to ensure DOTS in every case because patients may not come to the doctor regularly given our present socio-economic condition. Better implementation of DOTS is very much essential.
Again, the monitoring system of NTP is not very adequate and monitoring is essential for an effective NTP. In Bangladesh, the monitoring is done only from the capital but this central monitoring system may not bring effective results for us. So the monitoring system should be decentralized and carried out at the district level for better registration and case detection. Technical advice is needed for TB control programme. Consultants should go to the peripheral areas to make local people aware about the technical aspects regarding TB, its treatment and diagnosis.
Abdul-Muyeed Chowdhury, Executive director, BRAC: Let me clarify on the performance of the BRAC Shasthaya Shebika. BRAC deals directly with the patients within BRAC's operational territory. The patient has to deposit 200 Tk as bond money and the entire deposit is refunded to the patient after completion of treatment. The Shasthaya Shebika gets a small incentive from the BRAC fund.
Shasthaya Shebika regularly supervises and monitors the drug intake situation of the patients. Therefore, to make the NTP programme successful, the government has to create an efficient and effective monitoring team at the regional level
Dr. Salehuddin Ahmed, Pro-vice Chancellor, BRAC University: GO and NGO partnership has been developing since 30 years but they often ignore each other. It is very easy to say that we should function through Public Private Partnership but it's much more difficult to implement it. We have to find better mechanisms for better collaboration. The rule of each partner should be specifically identified and they should perform their responsibility properly and all this should be monitored.
Financial support is very important to make this programme successful at the grassroots level. Again Social Mobilization is very crucial for the success of the programme and it should start from the grassroots level by the Shasthaya Shebika. Most of the benefits of the communication, mobilization and community advocacy programme reach only the top 50 % people of the society.
Dr. Frank Paulin, Health Advisor, DFID: A major problem which contributes to higher disease spreading in South Asia as well as among Bangladeshis is spitting. It means we need to address social behaviour issues more stringently. For controlling TB, effective treatment and case detection are both important. We have to try and achieve a case detection rate of 70% within the next few years.
Dr. M Amanullah, MP and Ex-State Minister for Health, Member, Health Standing Committee: Our main problem is poverty. At first, we have to reduce the poverty level and then deal with other issues. To make NTP programme successful we have to give equal emphasis on the improvement of social condition, economic condition, living standard, housing, drainage, sanitation, and environmental issues all over the country. All these facilities should not be available only to the well off sections of society. They should be accessible to all but more so to the low-income groups, people who live in the slums and to the squatters. TB is a disease of poverty.
Dr. Dinesh Nair, Health Specialist, World Bank: Sustainable and long-term management of tuberculosis programmes will improve the entire health scenario in this nation. For long-term sustainability we have to improve the capacity of monitoring, supervision, advocacy and health service delivery system. In case of Public Private Partnership, the organized private sectors such as the NGOs are playing a vital role for controlling tuberculosis.
Dr. K. Zaman, Scientist/ Epidemiologist, ICDDR,B: ICDDR, B collaborates with NTP and BRAC on health issues. We need precise information about TB from both urban and rural areas. Prevalence of TB is a major issue in Bangladesh. It has been observed that about 95 persons out of 100 thousand (100,000) are infected by TB (research was conducted on a population of those over 15 years of age) in some specific areas. The diagnosis of children with TB is difficult because they cannot produce sputum.
Dr. Shaila Rodrigues, Second Secretary, CIDA, Canadian High Commission: I would specifically emphasize on the supervision system, which is necessary to improve the quality of TB control programmes. The Government of Bangladesh is working hard for the success of the programme and is achieving the target. I would also emphasize on increasing the cure rate and maintaining it. CIDA is working with International Union to control vulnerable diseases. I would suggest strengthening of the Public Private Partnership with more private involvement, and more NGO activities like BRAC's pilot projects on TB and building up a linkage between HIV and TB controlling projects.
Dr. Sadia Dilshad Parveen, Director, Quality Improvement, NGO Service Delivery Program: In Bangladesh, case detection and cure rate improved in the mid 90s. Basically it was possible due to increased donor support for the TB controlling programme. Without developing human resource and capacity for maintaining the case detection rate, it is not possible to achieve success in TB control programme. The goal of the NTP programme is to achieve 70% case detection rate within the next few years. Maximum donor groups provide technical support such as drugs, treatment options and infrastructure. But we need systemic improvement, instalment and maintenance for TB programmes.
Social mobilization is also important for this programme such as social interaction and making available information about TB treatment to the general people.
Robert J. Timmons, Chief of Party, NGO delivery programme (NSDP): TB programmes have gained substantial progress in the past few years. It is a challenge for Bangladesh. If the donor groups fund such projects, those programmes will run longer. The European Commission has many developing partners in the health sector. They have provided substantial support to Bangladesh. At the same time they are also the major contributors of the Global Fund. Co-ordination among the partners and donor groups are necessary. The regulatory activities should be carried out by the State.
Mohammad. Iqbal, Project Director. Urban Primary Health Care Project (UPHCP): My concern is about the ACS (advocacy communication and social mobilization) aspect of the programme. We have very little communication with the people who are living next door or for that matter in the slums. I would therefore prefer mobile advocacy team in the deprived areas to motivate the people about TB and inform them through sign boards. Our information and communication system should also be developed for greater impact. Electronic media and mobile teams may not reach all levels of people. We should also develop an appropriate website on health where all kinds of information is available and also have a provision to share the information with others.
I propose government academia and NGO partnership side-by-side with the GO - NGO collaboration. I would also add the expansion of primary health care project in every urban area as well as the City Corporation. If their achievements in delivering public health are noted and recorded carefully this will be a good example for others to follow.
Dr Makhduma Nargis, Vice President Bangladesh Mohila Parishad: Existing data shows that males are more affected by TB than females. But females might be prone to infection by tuberculosis than male. They may be tested less. Along with sputum tests I would emphasize on other diagnostic procedures.
The garments workers are very vulnerable to tuberculosis. Steps should be taken for proper case detection and treatment. Counselling is very important for controlling and treating TB.
Dr. Obaidur Rob, Country Director, Population Council: Vital registration system should be introduced in the NTP to find out accurate statistical data which is the key to control. The Health department of the government will be the main actor, not the NGOs. We must reform our health sector otherwise our next generation will not survive. The whole TB programme is a vertical programme which requires further examination for improvement.
Faruque Ahmed, Director, BRAC Health Programme (BHP): Sustainable political commitment is the prime issue for the success of NTP. This can be ensured through two ways. First, by mobilizing resources both domestic and international and Second, by mobilizing the partnership programmes. In Bangladesh the national budget is not adequate for the health sector. The government allocates lesser budgets for education and health than for defence. Another issue is that the government officials may not utilize this budget efficiently or put it in the right places. I propose local partnership, share resources and more advocacies at the national level.
Monitoring at local level especially in district and sub-district level is needed for successful sustainability of TB controlling programme. I also propose that as owners of garments industries have a significant role to play on TB controlling issues, they should be part of the Partnership.
Dr. Asif Mujtaba Mahmud, Associate Profrssor, Respiratory Medicine, National Institute of Diseases of Chest and Hospital: Over the last three years, the Government of Bangladesh is not associated with “World TB Day”, perhaps, because, it is not on the government's priority list. The NGO and other partners like BRAC have kept World TB Day going. The media also focuses on TB only occasionally. WHO focuses on TB Days in cities like Paris, New York, etc, but not in Bangladesh. I recommend creating focus on World TB day on the government priority list. Celebrities from the younger generation may act as ambassador who will convey the message to the people. Media has to play its role in creating this priority.
Afsan Chowdhury, Director, Advocacy and Human Rights Unit, BRAC: I would emphasise on both national level policy making advocacy activities and behavioural change related actions at the field level. Both need to be conducted and with equal emphasis. BRAC has conducted 3 small pilot advocacy projects in the rural areas and initial outcomes are positive. I strongly recommend more emphasis on Partnership which is a critical issue. We must recognize that the existing partnership is not adequate and we must work towards building a more effective one.
Prof. Dr. Mirza Mohammad Hiron, Associate Professor, National Institute of Diseases of Chest and Hospital (NIDCH): There are several delivery modes. BRAC is implementing the DOTS by the Shasthaya Shebika and different organisations are implementing the same through village doctors. They are treating about 35% of the cases. The treatment activities are the task of the village doctors not of the Shasthaya Shebika who monitors the side effects of drugs. BRAC staff is doing sputum smear examination but the rest 45% who have developed extensive tuberculosis go to private practitioners for treatment. I would also like to ask why BRAC has not involved doctors or technicians to control the tuberculosis.
Abdul-Muyeed Chowdhury, Executive Director, BRAC: In response to the health service provider issue (whether Community Health workers are good for TB programme) raised by Dr. Hiron, I would say that it is a question of resources, not just money but also human resources. Today, we are dealing with 35% smear positive tuberculosis cases. The rest 65% will automatically come forward.
Dr. Zafrullah Chowdhury, Projects Coordinator, Ganoshasthaya Kendro: The Government has to produce drugs for TB cure that will be more cost effective. If we ourselves produce the drugs, it will cost say Tk 200 per month compared to Tk 1000 per month now The Government has to force pharmaceutical companies to produce TB drugs. Medical officers as well as students should have clear knowledge about TB and necessary steps and training should be taken for this. Socializing the health issue rather than medicalizing it will ensure sustainability.
Major General Dr. A.S.M Motiur Rahman (Rtd.), Chief Advisor of national HIV/AIDS programm and Chairman, Technical committee, National Aids Committee: On the matter of MDR (Multi-drug Resistant) TB, I think the doctors, private practitioners and clinics have responsibility for its advocacy. I would also suggest creating linkage among the disease control programmes such as HIV/ AIDS and Tuberculosis.
Tahmina Aziz, Director, (MBDC and Line Director-TB and Leprosy Control Program): I would recommend we take aggressive approach for TB control which would be very helpful for us. The approach of all sectors of private practitioners, hospitals, educational institutions, community peoples, community leaders, political leaders and imams (clerics) should be addressed.
I would however differ in my opinion with Obayedur Rab. The tuberculosis programme is not a vertical programme. At the same time I propose the integration of other health programmes with tuberculosis control programme. I would also like to add that the family planning issue should be given the same priority.
Dr. Khandoker Ezazul Haque, National Consultant, WHO: I would suggest the implementation strategy of partners who are working on the same issue. Dr. Viqarunnessa may explain about homogeneous strategy and guidelines not only for advocacy, communication and social mobilization but effective implementation of whole programmes, monitoring system and for evaluation.
Damien Foundation gives emphasis on village doctors but BRAC gives emphasis on Shasthaya Shebika. In this circumstance I propose strong advocacy for developing a homogeneous partnership system which will ultimately help us in effective implementation.
Prof. Dr. Md. Mostafizur Rahman, Director and Head, Department of Respiratory Medicine, National Institute of Diseases of Chest and Hospital (NIDCH): Due to lack of knowledge and awareness, people take drugs without consultation with a specialist. And sometimes they suffer from the side affect of wrong treatment. About 60 to 80 patients who are admitted to hospitals are suffering from MDR-TB. This MDR-TB creates another MDR-TB case which will not respond to the conventional TB drug. In our country for the diagnosis and treatment of MDR-TB there is no laboratory facility.
Dr. M. A. Hamid Salim, Country Director and Medical Advisor, Damien Foundation, Bangladesh: I would like to clarify about the village doctor's involvement at the community level. We have trained 13 thousand village doctors whose task is to only identify TB suspect cases. In each Union we have identified 6 DOTS providers who are proving DOTS to the patient. These village doctors are not directly involved with the diagnosis or prescribing drugs to the TB patient. The diagnosis and treatment are done only at the Upazila Health Complex. The village doctors are only facilitating access of suspect cases at the community level & providing DOTS at the community level to ensure compliance with the DOTS regime.
Runia Mowla, Coordinator, En-gender Health: The gender aspect of DOTS management must be examined and addressed. There is no special attention to women and many women may be kept away from treatment of any disease because of our poor social and economic situation.
Concluding remarks by Dr. Vikarunnessa Begum:
At the end of the discussion session, Dr. Vikarunnessa, responded to some of the issues raised.
On the question of Sustainability of the NTP programme we have integrated the TB control programme with general health service and it is not a vertical programme. At the Upazila level we have trained 1 doctor and 1 Medical official and conducted 6 days basic training course for the laboratory technician to learn diagnosis and examine the sputum. We also provide 3 days training to the mid level worker and the field level worker for 1 day. Without giving training they do not start any DOTS any where. This basic training is pre-conditional to the initiation of DOTS.
All those facilities are provided by the government for the upazila level but not for the NGOs. For ensuring sustainability of the TB control programme in future, we will start the peripheral laboratory chain in the country to develop capacity.
For Supervision and monitoring issues, we have organized a training programme to the junior consultants with USAID assistance. We have trained them for 3 days in different batches on supervision and monitoring of the NTP programme. We have also developed district level supervisory team which includes the district Civil Surgeon. The district level peripheral team will supervise the upazila level and observe how the programme is running as well as the treatment pattern of the patient. The team members will first educate the patient and then start the treatment. For this reason the treatment success rate has reached 90% in DOTS.
The NTP also has prepared a plan to involve the family welfare assistants (FWAs). We have also decided to incorporate TB programme in the curriculum of medical students, nursing student and others. All those activities will help sustain the programme.
On the question of treatment and diagnosis facilities for garments workers in different industries, we are performing some activities jointly with other NGOs in some garments factories but not as a sectoral activity.
Finally, she discussed about the cost of medicine. NTP is getting about 50% of the drug as free. 25% is coming from the government and 25% from the Global Fund.
Summarising the workshop, the Editor of The Daily Star Mr. Mahfuz Anam said that the roundtable was on a subject of great concern for all. Should the TB situation fail to be arrested there could be a health catastrophe beyond our ability to contain. To prevent such a situation he called for a national alliance, which would go beyond the Government and the NGOs and the donors.
Mr. Mahfuz Anam then said that he was pledging full support of his paper and that he would personally be involved in any initiative, which could improve the situation concerning TB in Bangladesh.
Mr. Abdul-Muyeed Chowdhury thanked the Daily Star for its support in holding the roundtable and also for extending support to the fight against TB.
The meeting was declared over after this.