|
Info-tech
The modern approach of assisted reproduction
Steps in the Treatment of Infertility
Dr Cheng Li Chang
The desire to mate and reproduce is one of the strongest driving forces in nature. This strong and often obsessive drive can cause much stress and confusion in wisely choosing when and what to do when pregnancy fails to occur.
In my daily practice, I am struck by the fact that many couples did not realise that they had a problem, resulting in a delay when seeking medical attention. There are also many who go from doctor to doctor hoping to find the 'magic' solution, resulting in a wasteful repetition of investigations and a delay in starting effective treatment. At the other end of the spectrum, there are also couples who request infertility treatment even before there is a problem.
As a simple rule-of-thumb, the urgency to seek medical attention hinges on three factors, firstly, the age of the woman; secondly, the length of time trying to conceive and thirdly, the presence of a medical problem.
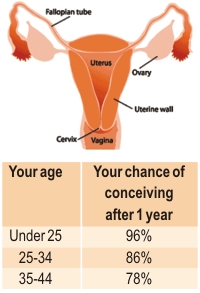
The single most important factor that affects fertility is the woman's age. Fertility is fairly stable until the age of 35 years of age. Thereafter, there is a gradual drop in fertility. By 40 years of age, the drop in fertility is profound. It is therefore of utmost importance that women who are coming to 35 and have not been able to become pregnant, to seek medical attention soon. This becomes urgent for women who are fast approaching 40 years of age.
Secondly, once you have decided to have a baby, it is easy to become concerned if you don't conceive in the first month you try. But the fact is, the chances that a normal, healthy woman (below 30) regularly having intercourse, will only have a 20 to 40 percent chance of falling during any given cycle.
So, what has gone "wrong" with the other 60 to 80 percent of women who failed? Most of the time, there is no medical reason, and the cause is usually because the quality of the egg or sperm is too poor to achieve fertilisation, or that fertilisation occurs but the embryo does not survive beyond a few days. In fact, the odds that you will conceive are actually quite good once you look at them over the span of a year of unprotected intercourse, according to data from the National Center for Health Statistics in USA.
In the absence of any medical problems, women below the age of 30 should see a gynaecologist after one to two years of unprotected intercourse. However, those between 30 to 35 should seek attention after six to nine months. The urgency increases in women between 35 and 40 if they are not pregnant after six months; while women over 40 should seek attention after three months of unsuccessful trying.
In most instances, your gynaecologist should be able to perform a preliminary fertility work-up and treat most of the problems. If you have not conceived under a doctor's care within six to 12 months, see a fertility specialist (also called an RE specialist, who is a gynaecologist with additional experience in fertility management), who can guide you through the plethora of treatments.
You should actively participate in your treatment and assist your RE Specialist in formulating a logical plan to achieve a pregnancy.
Steps in fertility treatment
Preliminary evaluation and fertility tablet (Clomiphene)
The first step if there is no pregnancy after the recommended time limits is to see your gynaecologist. Some preliminary tests will be done which will include blood tests, ultrasound scans and a sperm analysis. S/he will probably give you a course of fertility tablets called Clomiphene. This will ensure that you ovulate. If a pregnancy does not occur within six months, then further continuation of Clomiphene is unlikely to result in a pregnancy.
Checking the tubes
We would normally consider checking the fallopian tubes next. The preferred way is through an operation called a laparoscopy. This involves inserting a small telescope into the abdomen through the navel. This has the advantage of checking if the internal organs are normal and healthy, whether the tubes are blocked and if the ovaries are close to the 'mouth' of the tube.
 Super-Ovulation and Artificial Insemination Super-Ovulation and Artificial Insemination
Super-Ovulation and Artificial Insemination (SO-AI) is the second step in treatment. This involves daily hormones injections to 'give a boost' to your natural hormones. This has the aim of inducing the growth of up to three eggs. At the time of ovulation, your husband's prepared sperm will be put into your womb in a simple and painless procedure. We do not recommend pursuing this method if there is no pregnancy after four cycles of treatment.
In-Vitro Fertilisation
In Vitro Fertilisation (IVF) or more commonly called the 'test tube baby programme' is the next step of treatment if SO-AI fails. It is the preferred step if the fallopian tubes are blocked or when there is insufficient sperm for SO-AI. It basically involves extracting eggs from the body and mixing it with sperm in the laboratory. Three fertilised eggs, now called embryos, are replaced in the womb.
The complexity of IVF lies in ensuring that the egg development occurs at the correct speed, and to determine when they reach maturity. This is because immature eggs do not fertilise.
IVF usually require the combined and frequent use of ultrasound scans and blood tests to determine when the eggs are mature. One can expect an average of up to 70 injections over a four week period, and about 15 visits to the clinic. During these visits, blood tests are usually done to measure hormone levels. A period of hospitalisation may be required after the eggs are retrieved.
Simplified IVF at Thomson Fertility Center does away with almost all the blood tests. The number of injections are reduced to a minimum on average 15 injections over one month are required in comparison to 70 injections in other IVF centres. This allows the number of visits to be reduced to about 8. Hospitalisation is rarely required. All these can be achieved with no reduction in safety and pregnancy.
The Thomson philosophy
Simplification is part of the overall philosophy of holistic patient-centered management at Thomson Fertility Centre. The clinical philosophy is not one of blind pursuit of the latest advances, but one of selecting and integrating the appropriate ones to achieve the dual goals of excellence with simplicity for patients. It is, therefore, not related to any particular procedure or protocol.
Comprehensive patient education is the cornerstone of our philosophy. This ensures that you have a good overview of the various aspects of fertility treatment. A good understanding will allow you to be an effective partner in the planning of your fertility treatment. Important management decisions and problems can be discussed with your needs and concerns in mind.
Success rates
Success rates are often used to compare the quality of IVF centres. This is a common mistake as success rates are influenced by a multitude of factors. For example, a very good centre may have 'poor' results because they happen to attract and treat the most difficult problems. A mediocre centre may have very impressive results simply by preferentially treating young patients with minor problems. An excellent discussion on this topic may be found on the following site www.givf.com/success.cfm
IVF, like any medical treatment overcomes well-defined problems and aims to restore fertility back to what is naturally expected. Reputable centres tend to achieve success rates in the ball-park of what is naturally expected.
Choosing a fertility centre
Your choice of fertility centre is an important one and must be tackled in a methodical and comprehensive manner. First of all, do all the background checks on the track record and history of innovation. Centres that have been around for a long time have stood the test of time. Furthermore, a record of innovation implies solid basics. Ask your doctors who they would go to if they had fertility problems.
Secondly, contact the centre by phone and/or email to assess their responsiveness and forthrightness to your queries. Queries should be answered clearly and promptly. Do not expect, however, an in-depth assessment of your problem, because a proper assessment is beyond the capability of telephone/email communications.
Finally, visit the centre to get a sense of the 'look-and-feel' of the people and place. See the doctor and present your medical history with all available reports of previous test results that you can gather. He must be able to address all your concerns and answer your questions in a logical and easy-to-understand manner. Seek a second opinion if the answers given to you do not seem logical. You should have a basic plan of action by the time you leave the Centre, but it is best not to commit to any treatment until you have had some time to 'digest' the information given to you.
Take home message
Do not delay medical review by a Fertility (or RE) Specialist as age is of crucial importance in treating fertility. The following points well help you to decide when you should seek specialist advice urgently.
1. age more than 35 years
2. infertility for more than two years
3. irregular periods
4. sexual problems
5. previous abdominal operations
6. more than six cycles of Clomiphene
7. more than four cycles of SO-AI.
Dr Cheng Li Chang, MBBS, FRCOG, FAMS is a Medical Director of Thomson Fertility Centre, Singapore.
Copyright (R) thedailystar.net 2006 |