|
Cover
Story
What
Ails DMCH?
AASHA
MEHREEN AMIN and AHMEDE HUSSAIN
Photographs:
Zahedul I Khan
 The
Dhaka Medical College Hospital (DMCH) is the largest public
hospital in the country. For those who cannot afford the high
fees of private hospitals or clinics, the DMCH is the only
hope for getting cured. In the event of an emergency, it is
often the only option. Even patients from far-off places in
the country come all the way to DMCH in the absence of beds
or proper medical treatment in their own districts. But in
spite of its crucial role in our ailing health care system,
the DMCH is a house of endless horror stories. Rampant corruption,
years of unhindered politicisation of the entire institution
and an unrealistically poor budget have turned DMCH into a
hellhole for the sick. The
Dhaka Medical College Hospital (DMCH) is the largest public
hospital in the country. For those who cannot afford the high
fees of private hospitals or clinics, the DMCH is the only
hope for getting cured. In the event of an emergency, it is
often the only option. Even patients from far-off places in
the country come all the way to DMCH in the absence of beds
or proper medical treatment in their own districts. But in
spite of its crucial role in our ailing health care system,
the DMCH is a house of endless horror stories. Rampant corruption,
years of unhindered politicisation of the entire institution
and an unrealistically poor budget have turned DMCH into a
hellhole for the sick.
The first
thing that hits one in the face upon entering Dhaka Medical
College Hospital (DMCH), which looks more like a medieval
mansion in a gothic horror movie, is the noxious, suffocating
smell. It comes from a mixture of grimy floors, stale sweat
and general claustrophobia of this gigantic maze where inhaling
too deeply might make you faint. Pungent enough to make a
healthy person fall sick, it is the smell of gross negligence.
Signs
of utter disrespect for human life are everywhere. On a busy
day when the wards are all filled up, the corridors outside
are strewn with sick patients, men, women and babies, some
waiting to be healed, others waiting to die.
Nine-year-old
Tanvir lies sleeping on the floor outside Ward 35 with a bandage
on his head and a saline apparatus next to him. His father
informs us that Tanvir fell from the terrace of their flat
in Hosni Dalan. "We brought him here and after initial
treatment we had to take him home as they told us that there
was no bed," he says as Tanvir's mother keeps looking
at her son. But Tanvir's condition deteriorated that night
and his parents had to rush him back to the hospital. "We
have to buy all the medicine ourselves from outside. I got
mad because why should we have to buy all this when this is
a government hospital and is supposed to provide free medicine?"
Most of
the drugs the doctors at the DMCH prescribe come from government-run
Essential Drugs Company Limited (EDCL). Drugs that the EDCL
does not produce are bought in an annual open tender by the
hospital. Usually a purchase committee is formed to assess
the need for drugs the hospital has in each fiscal year. "But
nepotism and corruption rule most of the purchasing,"
says Zaman (not his real name), a Class Three employee. He
alleges that in most cases the doctors refuse to prescribe
the sub-standard drugs that the hospital has purchased through
its annual tender, thus forcing the patients to buy drugs
from the dispensaries outside DMCH. "Some Class Four
employees steal essential drugs and sell them to different
drugstores across the country," he adds.

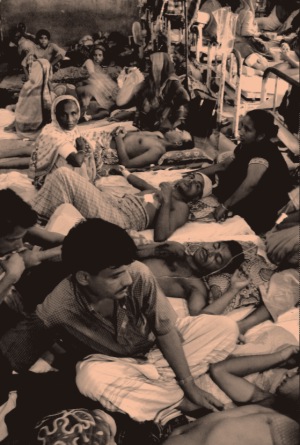
Failing
to get a bed many patients stay under the banister with their
attendants
According
to a senior official of the hospital administration, while
the DMCH has a supply of basic drugs and medical supplies
like syringes, gauze, saline, etc., some drugs such as expensive
antibiotics have to be bought by the patients because they
are not available at the hospital medicine store. The official
however, evaded the issue of drugs being stolen or sold off
outside the hospital.
Standing
in the corridor is a young woman trying to soothe her baby
-- just over a month old. Parveen Islam had to come all the
way from Chandpur when her newborn baby's stomach became abnormally
inflated. After being refused from Shishu Hospital and Mitford
Hospital because there were no beds vacant, she ended up at
DMCH, where, miraculously, she did get a bed. It took 10 excruciating
days of tests before the doctors diagnosed the problem: an
intestinal complication. "We had to do all the tests
outside because the tests done at DMCH are not accepted by
the doctors," says Parveen's brother.
 Encouraged
by Parveen, other people come forward and give their list
of grievances. "The nurses are extremely rude, especially
the younger ones," says Shaheen, whose niece is a patient. Encouraged
by Parveen, other people come forward and give their list
of grievances. "The nurses are extremely rude, especially
the younger ones," says Shaheen, whose niece is a patient.
"The
food the cooks give us is substandard and they never give
enough rice. We have to buy rice from the cooks for Tk. 5,"
she continues. Amanullah (not his real name), a ward boy,
echoes the allegation and has his own Pandora's box of the
evils committed in the hospital. According to him, the cooks
sell raw eggs and boiled eggs outside the hospital and cooked
food to the patients although food is supposed to be free
of cost. "The cooks themselves eat the best part of the
food and also give it to the hospital employees' union leaders
to keep them happy."
Food,
moreover, is not the only item sold to make a quick buck.
According to Amanullah, some doctors and nurses form an understanding
whereby the doctors over-prescribe drugs of a patient and
then the extra drugs are sold off. "Medicine is often
stolen by OT (Operation Theatre) ward boys, OT sisters and
even doctors," says Amanullah.
 But
the more obvious anomaly is the unbelievable filth in the
wards where many patients are critically injured. Several
weeks ago while visiting a patient -- a young garment worker
who had been raped and her spinal cord almost completely severed
-- we saw scores of little cockroaches all over the walls.
Some of them were running up the patient's body. The floor
where more patients were lying on was sticky with grime. Two
cats freely wandered around the wards, looking for scraps. But
the more obvious anomaly is the unbelievable filth in the
wards where many patients are critically injured. Several
weeks ago while visiting a patient -- a young garment worker
who had been raped and her spinal cord almost completely severed
-- we saw scores of little cockroaches all over the walls.
Some of them were running up the patient's body. The floor
where more patients were lying on was sticky with grime. Two
cats freely wandered around the wards, looking for scraps.
The stink
from the bathrooms waft into the corridors; the floors are
wet and muddy with discarded food strewn all over. "In
such unhygienic conditions how can sick patients survive,
especially those who run the risk of contracting infections?"
asks Shaheen.
"The
ayahs are supposed to clean everything," says
Sharmin, a patient's sister, "but if we don't give them
money they refuse to do it."
Class
Four employees, who include the Sweepers, Zamadars, and Sardars
are not transferable. This, Zaman believes, has given them
perpetual immunity from any administrative action for negligence
of duty. "They cannot be transferred as long as the case
is 100 per cent proven against them," says Zaman.
Class
Four employees have their own union, which is affiliated with
both the ruling and the opposition parties. And though the
union leaders draw their salary year in and year out, they
seldom lift a finger as far as work is concerned. "There
are seven ward-masters in the whole hospital, and around three
Sardars work under them," says Zaman. On an average,
he continues, a ward master has to supervise 150 people. "But,
most of them," Zaman alleges, "do not even turn
up at work." And like their supervisors, most Class Four
employees who work under them regularly shirk their responsibilities.
 The
DMCH administration turns a blind eye to this, as they are
large in number and most Class Four union leaders are involved
in party politics. "You can't do anything if a ward boy
or an ayah misbehaves with you. Once a Director General
reprimanded a sweeper for not cleaning the ward properly;
that DG was later transferred because his political power
outmatched that of the sweeper's," Zaman recalls. The
DMCH administration turns a blind eye to this, as they are
large in number and most Class Four union leaders are involved
in party politics. "You can't do anything if a ward boy
or an ayah misbehaves with you. Once a Director General
reprimanded a sweeper for not cleaning the ward properly;
that DG was later transferred because his political power
outmatched that of the sweeper's," Zaman recalls.
In fact
ward boys can hardly be seen at the Emergency Unit of the
hospital where they are supposed to attend to the patients.
In the absence of the ward boys, a gang of brokers, in connivance
with the Class Four employees, runs a thriving business of
luring patients to nearby private clinics. "After grabbing
the patients, the brokers huddle them into a waiting ambulance
to take them to the nearby clinic. Each broker usually makes
from Tk 4,000 to 6,000 a month. And the commission is about
Tk 200 for a delivery patient and Tk 500 to 1,000 for general
surgery like hernia, cleft-lip and minor burn," writes
Shamim Ashraf in a Daily Star report.
The list
of allegations is endless. Getting a trolley for carrying
a patient costs Tk 100; relatives have to pay Tk 1,000 at
the morgue to get the dead out of the hospital. Duties of
DMCH's Blood Bank are sold every night to outsiders who buy
blood from drug addicts. All the revenues earned are distributed
equally among different unions.
"Everyone
in the DMCH wants to work in the blood bank," says Zaman.
Other most sought-after departments, according to Zaman, are
Ticket selling, Pathology and Morgue.
During
one of our visits to the Emergency unit we witnessed several
individuals (including one of us) being charged Tk10 for an
admission ticket when the official rate printed in bold on
the wall was
Tk 5.50.
According
to an official who preferred anonymity, unless complaints
are in written form, there is little the administration can
do.
"We
have received written complaints from letters and we have
taken action against the employee concerned in the form of
a suspension or cancellation of his yearly increment or retaining
the salary. We have to get the name of the offender to do
anything," says the official.
 There
are worse horrors ahead. On Wednesday September 22 when we
enter DMCH, we are pleasantly surprised by the apparent clean
look in the ground floor corridors. The floors look reasonably
clean, the walls have been freshly whitewashed and miracle
of miracles, there are only faint traces of the formidable
smell that otherwise characterises DMCH. But it only takes
a flight of stairs up to Ward 35 to realise that nothing has
changed. Outside the corridor the body of a hit and run accident
is lying with a sheet drawn over the head. A man lifts the
sheet to see the mutilated face. He admits that he is not
a relative, or even a patient in the hospital. Just someone
randomly loitering around with morbid curiosity. Fatema Begum,
the relative of a patient says, the dead girl was a garment
worker who had been hit by a bus. "She was left here
all night without any saline and died at seven in the morning,"
she adds. There
are worse horrors ahead. On Wednesday September 22 when we
enter DMCH, we are pleasantly surprised by the apparent clean
look in the ground floor corridors. The floors look reasonably
clean, the walls have been freshly whitewashed and miracle
of miracles, there are only faint traces of the formidable
smell that otherwise characterises DMCH. But it only takes
a flight of stairs up to Ward 35 to realise that nothing has
changed. Outside the corridor the body of a hit and run accident
is lying with a sheet drawn over the head. A man lifts the
sheet to see the mutilated face. He admits that he is not
a relative, or even a patient in the hospital. Just someone
randomly loitering around with morbid curiosity. Fatema Begum,
the relative of a patient says, the dead girl was a garment
worker who had been hit by a bus. "She was left here
all night without any saline and died at seven in the morning,"
she adds.
At this
time it is already 2pm in the afternoon, i.e., over seven
hours. Right in front of the body, three other patients lie
helplessly in the corridors. One of them, a young woman called
Moina, is lying on a dirty piece of foam. It is hard to tell
whether she is sleeping or unconscious. Her attendant, a stranger
who happened to be in the same place as her when the accident
took place, says that Moina was hit by a double-decker bus.
During moments of lucidity she had given him her name and
the area where she lived. The man had paid for all the medicine
she needed but her relatives still had not been contacted.
 Opposite
Ward 35 is Ward 35A, which is cramped, dark and damp. Patients
and their attendants are jam-packed together, making the air
difficult to breathe. Again, the floor of the ward is covered
by scores of patients who are still waiting for beds. The
overnight facelift downstairs is attributed to the Saudi Arabian
Health Minister's recent visit to the hospital. Opposite
Ward 35 is Ward 35A, which is cramped, dark and damp. Patients
and their attendants are jam-packed together, making the air
difficult to breathe. Again, the floor of the ward is covered
by scores of patients who are still waiting for beds. The
overnight facelift downstairs is attributed to the Saudi Arabian
Health Minister's recent visit to the hospital.
Zaman
blames the utter indifference that is so palpable all over
the hospital, on the politicisation of the DMCH administration.
"If you do not support the ruling party you will not
be able to work in DMCH," he says. "Whenever a new
government comes to power, the first thing the health ministry
does is issue transfer orders," Zaman continues. "Opposition
party followers will be marked out, and they will be transferred
to far away places outside the capital," he explains.
In
fact, immediately after coming back to power in 1996, the
Awami League (AL) transferred many doctors to different mufassil
towns for their involvement with the then opposition Bangladesh
Nationalist Party (BNP). That deplorable practice was repeated
when the BNP came to power in 2001.
To make
matters worse, every doctor in the hospital is actively involved
in national politics. "All the appointments made here
are political," Zaman says. "There are some posts
that an opposition party-member can never hold," he continues.
According to Zaman all the Resident Physicians, General Physicians,
ENT Surgeons and Eye Surgeons are active members of the ruling
party and they were appointed by the health ministry. In most
cases, a doctor's skill, experience and training take second
place over political affiliation.
o why
is the most important hospital of the city in such a sorry
state?
 Low
salaries and lack of facilities contribute significantly to
the resentment among many DMCH doctors and nurses on government
payroll. Recently, around 73 nurses of DMCH (2,000 countrywide)
have not been getting any salary for the last four months
due to a bureaucratic glitch. But even in normal circumstances,
nurses feel they do not get paid enough for their services.
A nurse's basic salary is Tk. 2,225, and with rent and other
allowances included, it comes to about Tk. 4,900. Low
salaries and lack of facilities contribute significantly to
the resentment among many DMCH doctors and nurses on government
payroll. Recently, around 73 nurses of DMCH (2,000 countrywide)
have not been getting any salary for the last four months
due to a bureaucratic glitch. But even in normal circumstances,
nurses feel they do not get paid enough for their services.
A nurse's basic salary is Tk. 2,225, and with rent and other
allowances included, it comes to about Tk. 4,900.
"We
have no quarters and have to commute from far-off areas every
day," says Rahina Akhter, a senior staff nurse who has
been working at DMCH for the last 21 years. "Some nurses
come from as far as Gazipur and security is a big problem,"
adds Rahina, who is the Chairperson of Bangladesh Diploma
Nurses Association. Morjina Akhter, General Secretary of the
Association and also a senior staff nurse, adds that nurses
do not get other basic facilities like attached bathrooms
in the duty offices or a canteen to eat their meals or even
dressing rooms to change in. Supervisors are also very few.
There are only 31 supervisors for the 6,500 nurses at the
hospital.
Doctors
too, are ill-paid, especially considering their heavy workload.
A government-appointed Indoor Medical Officer (IMO) gets around
Tk. 6,800 at the entry level. Apart from regular duty from
8pm to 2:30am or 2:30am to 12pm, IMOs also have to do regular
night duty. Many IMOs therefore have private practices outside
DMCH.
"We
are not supposed to work anywhere else but how can we support
our families with such low pay?" says an IMO who now
gets around Tk. 8,000 per month.
 According
to the hospital's accounts section, DMCH's budget for 2004-2005
is 27 crore 18 lakh 79 thousand taka. This includes 2 crore
5 lakh taka for salaried first class employees, another 5
crore 92 lakhs for 'non-gazetted' employees, about 8 crore
taka in allowances and 10 crore 74 lakh 95 thousand in medical
supplies (including Medical Surgical Requirement, MSR) and
80,000 taka for vehicle repairs. An extra 23 lakh taka was
allocated to buy a car for a high official and 20 lakh taka
for office furniture. According
to the hospital's accounts section, DMCH's budget for 2004-2005
is 27 crore 18 lakh 79 thousand taka. This includes 2 crore
5 lakh taka for salaried first class employees, another 5
crore 92 lakhs for 'non-gazetted' employees, about 8 crore
taka in allowances and 10 crore 74 lakh 95 thousand in medical
supplies (including Medical Surgical Requirement, MSR) and
80,000 taka for vehicle repairs. An extra 23 lakh taka was
allocated to buy a car for a high official and 20 lakh taka
for office furniture.
But this
is only about 30 percent of the hospital's required budget.
According to the Accounts Officer, a proposal had been given
for a budget of about 78 crore taka but was brushed aside.
Apart
from lack of funds, officials at the hospital complain about
a severe shortage of manpower. The hospital has expanded from
800 beds to 1700 beds but the number of fourth class staff
has remained at 900. Now out of this number there are 367
vacancies.
 The
most pressing need at the moment is to have more beds. The
present 1700 beds are not enough, a dearth that leads to the
overcrowding on the floors of the wards with patients overflowing
into the corridors. "We try not to turn away any patients,"
says a high official of the hospital. The
most pressing need at the moment is to have more beds. The
present 1700 beds are not enough, a dearth that leads to the
overcrowding on the floors of the wards with patients overflowing
into the corridors. "We try not to turn away any patients,"
says a high official of the hospital.
"We
proposed an expansion of 600 beds two years ago. The government
has not taken the final decision yet," he says. "Medical
technology, in addition, has to be updated and for that you
need more funds."
 On
a regular busy day, the hospital is in a chaotic state with
patients taking up whatever space they can find, even under
the staircase. Every day at least 1,000 patients come to the
hospital's Outdoor Section. In crisis situations such as after
August 21st's bomb blast in Purana Paltan, staff at DMCH were
working round the clock and could barely cope with the rush
of severely injured people. Patients being left for days without
being operated on and acute shortage of blood were reported. On
a regular busy day, the hospital is in a chaotic state with
patients taking up whatever space they can find, even under
the staircase. Every day at least 1,000 patients come to the
hospital's Outdoor Section. In crisis situations such as after
August 21st's bomb blast in Purana Paltan, staff at DMCH were
working round the clock and could barely cope with the rush
of severely injured people. Patients being left for days without
being operated on and acute shortage of blood were reported.
Still,
in the case of an accident or any other emergency, DMCH is
the only place where patients are not normally turned away
as is the case in other hospitals and clinics. Its importance
for ordinary people cannot be emphasised enough. But unless
the government recognises the crying need of a major overhaul
of the hospital, whatever limited healthcare it now provides
the poor, will increasingly substandard.
Copyright
(R) thedailystar.net 2004
|